
Anatomy
The Temporomandibular Joint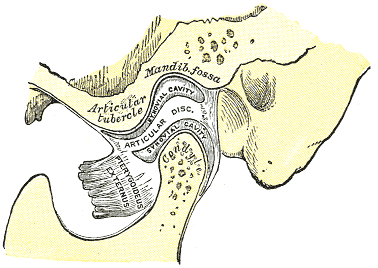
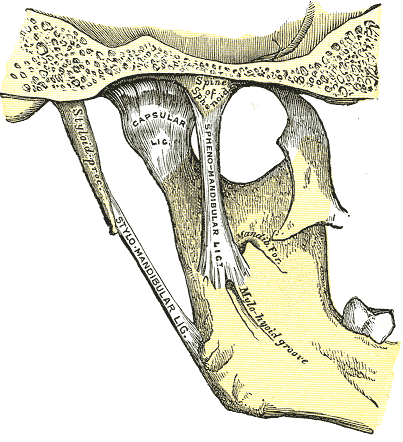
Ligaments
Movement
The TMJ is a ginglymoarthrodial joint meaning it allows for 2 types of movement; rotation and translation. Translational movement is the sliding of the joint allowing for protrusion, retrusion and side to side movement.
Rotation is the hinge movement of the joint and is an action mainly involving the inferior compartment. Translation is the sliding movement and an action of the superior compartment. To open the mouth you require both types of movement as rotational movement alone can only open the mouth to around 20mm, further movement cannot be achieved without translational movement of the joint. This is shown in the short clip at the bottom of the page.
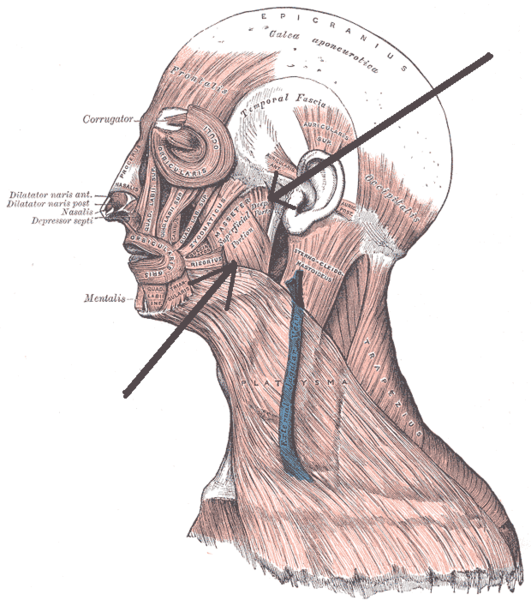
Muscles
· Masseter – Has 2 parts (superficial and deep portions). They arise from the medial surface of the zygomatic arch (deep) and zygomatic process of the maxilla bone (superficial). They insert into the ramus of the mandible (deep) and the angle of the mandible (superficial). The masseter acts to elevate the mandible (close the mouth) when contracted.
· Lateral pterygoid – Has 2 heads (superior and inferior). Originate from the infratemporal surface of the greater wing of the sphenoid bone (superior) and from the lateral surface of the lateral pterygoid plate (inferior). They insert into the articular disc of the TMJ (superior) and the condyloid process of the mandible (inferior). It acts to depress the mandible (open the mouth) and also translates the mandible from side to side.
· Medial Pterygoid – Also has 2 heads (deep and superficial). Originate from the medial surface of the lateral pterygoid plate (deep) and the maxillary tuberosity of the palatine bone (superficial). They both insert into the lower part of the ramus and angle of the mandible. Acts to elevate the mandible (close the mouth) and also translates the mandible from side to side with the lateral pterygoid and protrudes it.
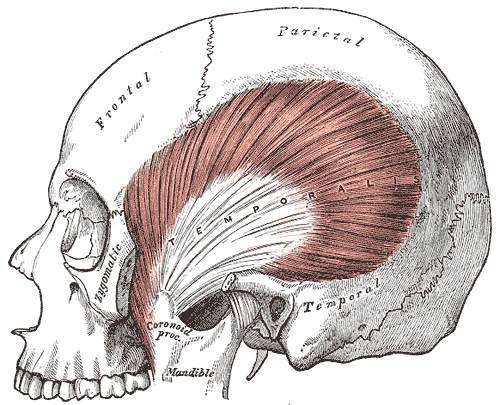
· Temporalis – Arises from the temporal fossa and inserts into the coronoid process of the mandible. Its action is to elevate the mandible (close the mouth).
Innervation, Blood Supply and Proprioception
All of the muscles of mastication are innervated by the mandibular branch (V3) of the trigeminal nerve (the 5th cranial nerve). The blood supply is from branches off the external carotid artery. Predominantly from the superficial temporal branch, but some other branches are also involved; deep auricular artery, anterior tympanic artery, ascending pharyngeal artery and maxilliary artery.
Proprioception of the TMJ is regulated by 4 receptors as shown in the table below.
|
Receptors |
Location |
Function |
|
Ruffini Receptors |
Capsule |
Position mandible (static) |
|
Golgi tendons organs |
Ligaments |
Protection of ligaments around TMJ (static) |
|
Pacinian corpuscles |
Capsule |
Accelerate during reflexes (dynamic) |
|
Free nerve endings (nociceptors) |
Capsule/Retrodiscal tissue |
Protection of TMJ (pain receptors) |